Playing Safe - COVID-safe music lessons
Guidelines for safer whole class music teaching during COVID-19, based on scientific evidence about virus transmission in enclosed spaces.
Guidelines for safer, whole class music teaching
The scientific evidence and the diagrams in this article are taken from two blogs by Erin Bromage, Comparative Immunologist and Professor of Biology (specializing in Immunology) at the University of Massachusetts Dartmouth. I urge you to read the blogs in full - please see References below for details.
Takeaway - Summary
When people share classrooms or other enclosed spaces for long periods of time without masks, one carrier can infect large numbers of the people present, whether or not physical distancing is practised. Infection happens via coughs, sneezes, speaking breathing, singing and touching, and the mechanics of these processes are explained in detail below. The potentially dire consequences are highlighted by two rather gruesome examples (Choir and Workplace).
The safest approach for music lessons is:
1. Make music outdoors wherever possible, keeping distancing
2. If playing inside, wear masks and ensure good ventilation
3. Wash hands and wipe down instruments with alcohol-based disinfectant before and after sessions and before swapping instruments between pupils within a session
The above guidelines are specific to music making and should be followed in addition to any general rules that make up overall school safety policy.
So percussion, stringed and keyboard instruments can be played safely in the classroom, providing masks are worn, ventilation is good, hands are washed and instruments are disinfected, but singing and playing wind instruments can only be done safely outdoors.
How the virus spreads
Social Distancing is only effective outdoors, or if you're just briefly inside a shared space indoors
Social distancing rules are really to protect you with brief exposures or outdoor exposures. In these situations there is not enough time to achieve the infectious viral load when you are standing 6 feet apart or where wind and the infinite outdoor space for viral dilution reduces viral load. The effects of sunlight, heat, and humidity on viral survival, all serve to minimize the risk to everyone when outside.
Importantly, of the countries performing contact tracing properly, only a single outbreak has been reported from an outdoor environment (less than 0.3% of traced infections). (ref)
Coughs and sneezes: the two main reasons why even 2m distancing inside isn't safe:
In order to get infected you need to get exposed to an infectious dose of the virus; based on infectious dose studies with other coronaviruses, it appears that only small doses may be needed for infection to take hold. Some experts estimate that as few as 1000 SARS-CoV2 infectious viral particles are all that will be needed (ref 1, ref 2).
A Cough: A single cough releases about 3,000 droplets and droplets travels at 50 miles per hour. Most droplets are large, and fall quickly (gravity), but many do stay in the air and can travel across a room in a few seconds.
A Sneeze: A single sneeze releases about 30,000 droplets, with droplets traveling at up to 200 miles per hour. Most droplets are small and travel great distances (easily across a room).
If a person is infected, the droplets in a single cough or sneeze may contain as many as 200,000,000 (two hundred million) virus particles which can all be dispersed into the environment around them.
If a person coughs or sneezes, those 200,000,000 viral particles go everywhere. Some virus hangs in the air, some falls into surfaces, most falls to the ground. So if you are face-to-face with a person, having a conversation, and that person sneezes or coughs straight at you, it's pretty easy to see how it is possible to inhale 1,000 virus particles and become infected.
But even if that cough or sneeze was not directed at you, some infected droplets--the smallest of small--can hang in the air for a few minutes, filling every corner of a modest sized room with infectious viral particles. All you have to do is enter that room within a few minutes of the cough/sneeze and take a few breaths and you have potentially received enough virus to establish an infection.
But it's not just coughs and sneezes that are the danger: if you're in an enclosed space with a carrier for a long enough time, you can still be infected by their breathing, speaking or singing.
A breath: A single breath releases 50 - 5000 droplets. Most of these droplets are low velocity and fall to the ground quickly. There are even fewer droplets released through nose-breathing. Importantly, due to the lack of exhalation force with a breath, viral particles from the lower respiratory areas are not expelled.
Unlike sneezing and coughing which release huge amounts of viral material, the respiratory droplets released from breathing only contain low levels of virus. We don't have a number for SARS-CoV2 yet, but we can use influenza as a guide. Studies have shown that a person infected with influenza can releases up to 33 infectious viral particles per minute. But I'm going to use 20 to keep the math simple.
Remember the formula: Successful Infection = Exposure to Virus x Time
But with general breathing, 20 viral particles minute into the environment, even if every virus ended up in your lungs (which is very unlikely), you would need 1000 viral particles divided by 20 per minute = 50 minutes.
Speaking increases the release of respiratory droplets about 10 fold; ~200 virus particles per minute. Again, assuming every virus is inhaled, it would take ~5 minutes of speaking face-to-face to receive the required dose.
The exposure to virus x time formula is the basis of contact tracing. Anyone you spend greater than 10 minutes with in a face-to-face situation is potentially infected. Anyone who shares a space with you (say an office) for an extended period is potentially infected.
And activities such as singing and playing wind instruments, which involve taking deep breaths in and forceful breathing out, increase the risks further.
Singing, to a greater degree than talking, aerosolizes respiratory droplets extraordinarily well. Deep-breathing while singing facilitated those respiratory droplets getting deep into the lungs.
Why masks are important
My mask protects you - Your mask protects me
Wearing a mask decreases the amount of respiratory droplets and droplet nuclei released in to the air. If we can decrease the amount of virus released into the air in droplets through wearing masks, we will increase the time in which we can have safer face-to-face conversations.
Masks - Wearing a mask while breathing, talking, yelling, coughing or sneezing catches respiratory droplets leaving your mouth and nose. Even with the most basic mask, virtually 100% of the large and medium-sized droplets are caught on the inside fabric surface. As the masks increase in quality, the amount of small respiratory droplets and droplet nuclei that get caught on the inside surface increases.
At a minimum, it is believed a good mask will reduce 50% of emissions from the mask-wearer. Multi-layered mixed fabric masks approach filtering efficiencies as high as 90% (Ref).
I want to emphasize that there is not clear evidence to indicate that cloth masks will protect you from inhaling the smallest infected respiratory droplets (those droplet nuclei) from another person. The primary purpose of a cloth mask, when worn by everyone, is to serve as a control for source emissions. If we lower the respiratory droplets coming out of us, we can substantially lower the amount of virus put into the air, thereby lowering the risk to everyone.
What about Bubbles?
Bubbles are only effective if you can be sure that all the members of the bubble are clear of infection at the outset and that they remain so. But where bubble members leave the bubble, mix with others (whether at school, on the way home, at home, or during other activities), and then return to the bubble, unless you test them before re-entry, you can't be sure the bubble remains safe. Masks and frequent hand-washing are vital, if your bubble isn't completely secure.
Gruesome Examples
Gruesome example 1. Choir: The community choir in Washington State.
Even though people were aware of the virus and took steps to minimize transfer; e.g. they avoided the usual handshakes and hugs hello, people also brought their own music to avoid sharing, and socially distanced themselves during practice. They even went to the lengths to tell choir members prior to practice that anyone experiencing symptoms should stay home. A single asymptomatic carrier infected most of the people in attendance. The choir sang for 2 1/2 hours, inside an enclosed rehearsal hall which was roughly the size of a volleyball court.
Singing, to a greater degree than talking, aerosolizes respiratory droplets extraordinarily well. Deep-breathing while singing facilitated those respiratory droplets getting deep into the lungs. Two and half hours of exposure ensured that people were exposed to enough virus over a long enough period of time for infection to take place. Over a period of 4 days, 45 of the 60 choir members developed symptoms, 2 died. The youngest infected was 31, but they averaged 67 years old. (corrected link)
Gruesome Example 2. Workplace Call Centre
A single infected employee came to work on the 11th floor of a building. That floor had 216 employees. Over the period of a week, 94 of those people became infected (43.5%: the blue chairs). 92 of those 94 people became sick (only 2 remained asymptomatic). Notice how one side of the office is primarily infected, while there are very few people infected on the other side.
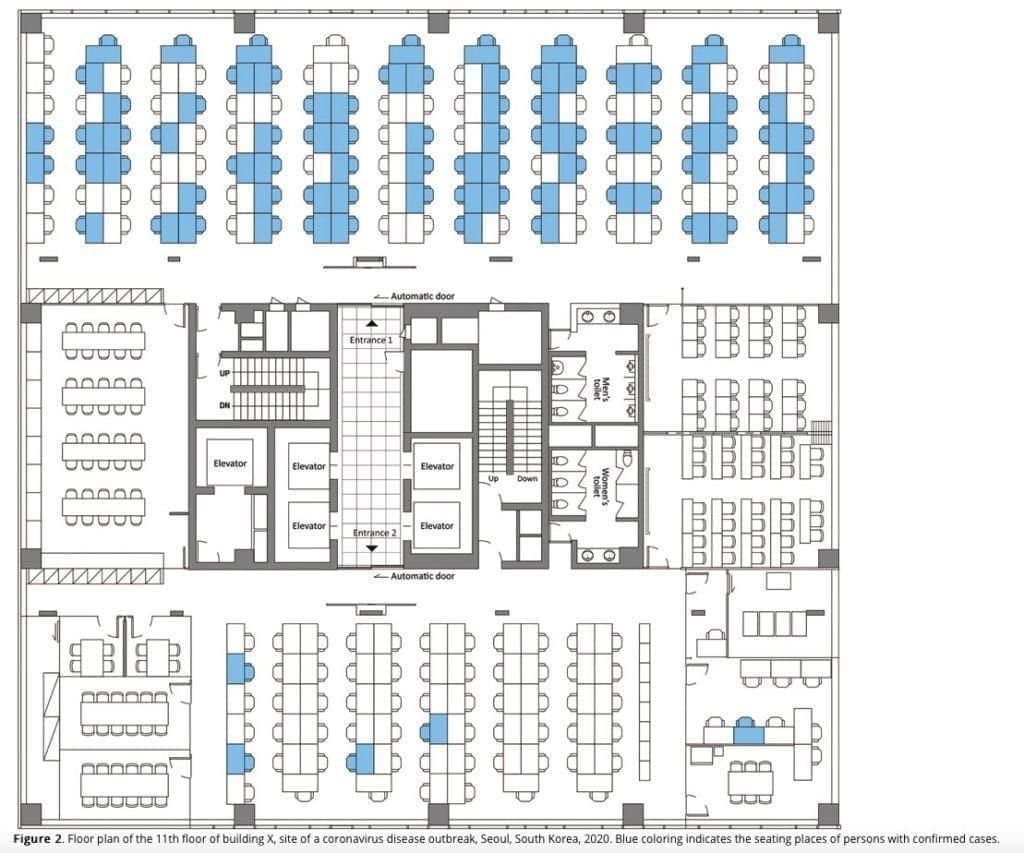
While the exact number of people infected by respiratory droplets / respiratory exposure versus fomite transmission (door handles, shared water coolers, elevator buttons etc.) is unknown, it serves to highlight that being in an enclosed space, sharing the same air for a prolonged period increases your chances of exposure and infection. Another 3 people on other floors of the building were infected, but the authors were not able to trace the infection to the primary cluster on the 11th floor. Interestingly, even though there were considerable interaction between workers on different floors of the building in elevators and the lobby, the outbreak was mostly limited to a single floor (ref). This highlights the importance of exposure and time in the spreading of SARS-CoV2.
The risks of sharing spaces can be summarised as follows:
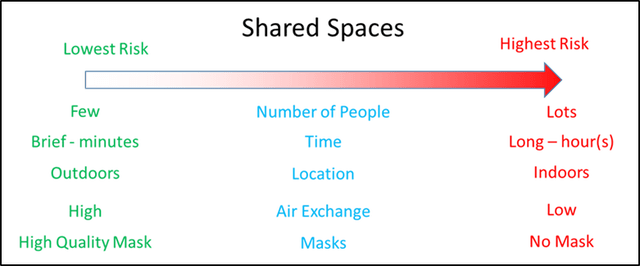
From The Risks - Know Them - Avoid Them by Professor Erin Bromage
What else can you do to reduce the risks?
Invest in high quality masks. Look for a mask that has a multi-layer multi-fabric design and an adjustable nose bridge to seal the top part of the mask to your face. The more of your exhaled air that is forced to pass through the mask fabric, the greater the filtering respiratory droplets will be caught inside the mask, and everyone is safer.
Improve the intake of outside air - the more air you can exchange with outside, the lower the viral burden in your space.
Improve the filtration - some HVAC systems can be easily upgraded to have high quality filters included in the system. Potentially upgrade with UV. Consider purchasing portable HEPA filtration systems for smaller spaces where the central system may not be adequate (therapy offices, treatment rooms etc).
References
All text in green and diagrams in this article are taken from two must-read blogs by Erin Bromage, Comparative Immunologist and Professor of Biology (specializing in Immunology) at the University of Massachusetts Dartmouth:
The Risks - Know Them - Avoid Them
My Mask Protects You; Your Mask Protects Me
I urge you to read these beautifully written blogs in full.
If you want to delve deeper into references, please see some of these links.
Prof. Adrien Birch. What's the Evidence on Face Masks? What You Heard Was Probably Wrong
Dr Jennifer Kasten at her facebook post here